Abstract
HCV virus has been a worldwide health-issue with noted expectancy ranging from 0.6% to 10% depending on geographical factors, and an estimated 71 million individuals worldwide are infected with this chronic virus. Diagnostic methods comprise HCV RNA test, Geno sensor, and laboratory testing, etc. With time there has been an immense number of advancements in HCV treatment. It started with the use of non-beneficial acyclovir to the introduction of interferons with incredible positive effects to cure hepatitis C patients. In this paper, we will review various classes of anti-HCV medications (PEGylated Interferon/RBV, DAA, and HTAs). Nanotechnology is a hallmark in the latest therapies involved in the management of HCV sufferers. WHO, in its Global health sectors strategy on viral hepatitis 2016-2021, hopes to reduce the spreading of this virus by 90% up-to year 2030.
Key Words:
Hepatitis C Virus, Genotype, Electrochemical Immunosensors, Geno Sensor, Vaccination, Nontechnology
Introduction
Hepatitis is an inflammatory state of the liver. It is normally achieved by a viral infection; however, other possible explanations for hepatitis can also be there. These include autoimmune hepatitis and hepatitis that happens as an auxiliary after prescription’s effects, medicines, toxins, & alcohol. Autoimmune hepatitis is an infection that happens when your body makes immunoglobulin contrary to your liver tissue. Hepatitis C happens by the HCV and is inherited via getting in touch with a contaminated body, normally via syringes and by contacting sexually. (Pawlowska, Sobolewska-Pilarczyk & Domagalsk, 2018).
HCV disease is global health trouble through an expected frequency ranging from 0.6% to 10% reliant on geographical factors and a predictable 71 million population globally with a persistent form of the disease. In Western Europe, the predictable incidence is 1.5% to 3.5%; however, in the UK, it is 0.5% (Tucker & Team, 2017). Persistent HCV is related to greater than before incidence and fatality and is a principal reason for last level cirrhosis with hepatic cancer globally. even though HCV disease seldom plays a part in incidence in children besides, some research studies show that HCV may compromise children’s life quality and performance, as the cognitive ability is compromised, and people report greater than before tension which compromises dynamics of the people and welfare. (El-Shabrawi, 2013).
Continuously affecting by HCV is a global therapeutic state affecting 71.1 million persons and resulting in globally 700 000 losses annually. Hepatitis C virus or HCV related disease difficulty is on rising as the educated population advances to belatedly stage hepatic diseases, which include carcinoma, imbalanced cirrhosis, and hepatocellular cancers (HCC). (Irving et al., 2012)
The alpha type of interferon is a type of proteins that contains oligosaccharides which have the main role in the therapy of chronic HCV and is well-thought-progress like interferon related processes, adapted forms of ribavirin siRNA with (IRES) blockers, NS3 and NS5a blockers, and original immunomodulators out the main part of therapy due to its competently potent immune system opposite to the virus, after that interferon combined with ribavirin becomes a gold standard. (McLauchlan et al., 2017)
Measurement of HCV Infection’s Markers HCV RNA Testing
Introductory contagion by HCV is described with the presence of infection in 2–14 days of contact & deliberate exposure of anti-Hepatitis C virus antibodies in 32–150 days of presentation (Wong et al., 2017). Commercial assays are accessible for identifying both anti-Hepatitis C virus antibodies and HCV RNA (Chevaliez et al., 2017). Among individuals presented to Hepatitis C Virus contamination, 25% would become suddenly pure contamination in the initial 6-12 months after exposure (Micallef, Kaldor & Dore, 2006) and would be unnoticeable for Hepatitis C virus RNA; however, most of them shall have recognizable anti-HCV antibodies that endure lifelong. Subsequently, a corroborative Hepatitis C virus RNA test is needed for sensing lively disease. Impulsive clearance occasionally happens after the beginning of a long-lasting infection (~6 a year postexposure), and in this way, a positive HCV RNA result from a long time after exposure is satisfactory for affirming chronic disease (Grebely et al., 2014). Hepatitis C virus RNA’s test, comprising of PCR- based assays and the branched-DNA (bDNA) test, used for healing checking or indications/symptoms. (Urdea et al., 1997)
HCV Antibody Test Positive Hepatitis C Virus Core Antigen (HCV cAg)
Unique Characteristics of HCV Diagnosis in Newborn Testing in Youngsters
By and large, testing for HCV disease ought to happen in all kids suspected to be "dangerous".
However, novel to kids is the arrangement of testing prescribed for newborn children destined to moms with HCV infection and those in danger of receiving infection. Moms having HCV shall have to flow anti-Hepatitis C virus immunoglobulin G, that cross placenta and may be estimated within the serum of newborns. Maternal antibodies can persevere in youngsters longer than twelve months; subsequently anti-Hepatitis C virus testing in newborn children no longer educational during this period. The American Academy of Pediatrics' recommendations’ proposals needs to postpone estimation of anti-Hepatitis C virus antibody. Infants 2 months old are reliable for this test (Perkins, 2006).
Cloning of HCV Infection Genome
Hepatitis C infection (HCV) genome’s cloning has been a gigantic development in the advancement of analyzing, detection, and observing HCV-contaminated sufferers. For the screening of blood donations & for diagnosing and affirming Hepatitis C virus, serological tests comprising of Enzyme-Linked Immunoassay and RIBATM strip immunoblot assay are fundamentally used.
Electrochemical Immunosensors for HCV Detection
Immunosensors are instruments that couple immunochemical responses in fitting transducers. By and large, an immunosensor comprises of detecting component & transducer. The benefits of immunosensors are identified with choosiness and the ability of the antibody-analyte binding reaction. These instruments are answerable for changing specific (Ab-Ag) interactions into quantifiable piezoelectric (Webb, Ravikumar & Rubinsztein, 2004) acoustic (Krishnamoorthy et al., 2008) electrochemical, magnetic, or optical signals & widely read for clinical diagnosis. (Pei et al., 2013). Electrochemical immunosensors are used in the identification of HCV core antigen.
Another electrochemical sensor, eSensor® HCV Genotyping Test (Zhang et al., 2013), was proposed to be used in typing and subtyping of Hepatitis C virus 1a, 1b, 2a/c, 2b, 3, 4, 5, and 6a/b.
Electrochemical Geno Sensors for HCV Monitoring
Geno Sensors
Geno sensors are used as alternatives to determine a series of components to assess the harm of molecules of DNA and appropriate devices aimed at examination of DNA for detecting sicknesses.
Geno Sensors Provide High Sensitivity
DNA hybridization technology is used aimed at diagnostic tests, less price, and performance’s ease. Though, a diversity of methods can be occupied for detecting Hepatitis C virus DNA hybridization. (TELES & FONSECA, 2008)
Laboratory Testing
There are major classes of assays that are serologic
assay, molecular assay, and genotype assay.
Serologic Assays
It senses specific antibodies to anti HCV by utilizing immuno-assay, anti HCV sense in the plasma or serum. By the US FDA, two immune enzyme assays are Abbott HCV EIA 2.0 & ORTHO HCV version 3.0 ELISA, also one upgraded CHEMILUMINESCENCE Immune Assay. The identity of the present EIAs is more prominent than 99%. At the point when we perform a test among those individuals having low commonness of hepatitis C, false-positive results happened. False-negative outcome happens in extreme immune separation, i.e., solid organ transplant recipient, contamination with HIV or in patients with hemodialysis (Hoofnagle, 2002; Hu and Tong, 1999; Preiser et al., 2000)
Molecular Assay
It identifies virus nucleic acid. This is a qualitative assay and more delicate than a quantitative assay. The accessibility of Transmission Mediated Amplification Assay and PCR based examine diminished the requirement of the qualitative assay (Fried, 2002)
Genotype Assay
This assay is typically performed in the clinical study, and epidemiological studies consider deciding the treatment. Six significant genotypes of HCV are: Genotype 1 is trailed by genotypes 2 and 3. Genotype 1 is the best- known in the US. Genotype 4 and 6 are among more uncommon genotype because of their developing culture in the US (El-Zayadi et al., 2005)
Figure 3: Showing Laboratory Testing
Hazardous Hepatitis C Virus Testing
a. Once this test is done for individuals under eighteen years having an extended threat of HCV tainting.
b. Episodic recurrent of this test would be available for individuals having an extended threat of HCV presentation.
c. Yearly Hepatitis C Virus investigation would be proposed for individuals implanting medications or HIV tainting. (Ghany & Morgan, 2020)
Hazard Based HCV Screening
Once, hazardous HCV screening was suggested for individuals under eighteen ages through recent/ ancient performances or introductions related to an extended threat of Hepatitis C virus sickness. There is, as of now, inadequate indication that infants take help from Hepatitis C screening. People having HCV infection remain unprotected though long the conduct, introduction, condition, or circumstance proceeds, thus justifying intermittent recurrent HCV testing. (Chou et al., 2020)
Anti-Hepatitis C Virus Drugs
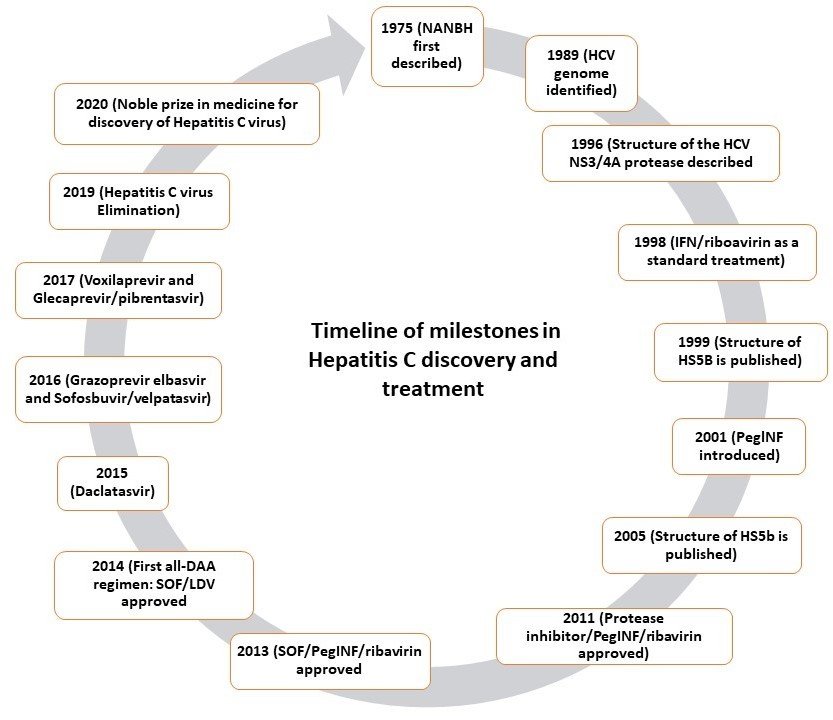
Earlier than 1989, HCV was not identified, and it was known as NANB hepatitis (Choo et al., 1990). acyclovir has been used at that time to treat NANB; even it was not beneficial. (Pappas et al., 1985) After that, interferons (IFNs), which were beneficially used to cure hepatitis, completely had a positive effect on NANB hepatitis. Interferons (IFNs) are signalling proteins, which are on the loose in the human body in reply to various infections (Marie et al., 2013).
Lying in 1991 and after the HCV’s identification, the United States FDA approved IFN-? as the primary anti-HCV medicine, and the use of INFs alone led to relapse and low sustained virological response rate.
Diverse studies were applied to achieve the proper drugs, dose, and extent of management to accomplish high sustained virological response.
In this assessment, anti-HCV medications have been arranged into three parts as below:
PEGylated Interferon/RBV
PEGylated interferon/RBV were accepted after stoppage of INFs treatment alone by the FDA.
This led to achieving high sustained virological rates (34% after every 6 months, with 42% after 12 months of cure) (Poynard et al., 1998). Moreover, improved SVR was accomplished through PEGylation of interferons (adding up of polyethene glycol). PEGylated interferon has a longer flow time and leads to a positive SVR rate, which was high when mixed with RBV (Lindsay et al., 2001; Reddy et al., 2001).
FDA accepted a mixture of PEGylated-IFN and PEG-IFN/RBV in 2001. The 6–12 months régime was taken as the ordinary one awaiting 2011 (McEwan et al., 2015). Despite the achievement of this mixture in eradicating the virus, some virus genotypes were not effectively treated and were directed to the evolution of new anti –Hepatitis C virus drugs, for example, DAAs (Poenisch et al., 2010; Pawlotsky et al., 2015).
DAA
DAAs means it directly acts on the HCV itself, specifically acting on certain stages in its life cycle. According to the method of the act and viral targeting (enzymes or proteins), four classes were developed:
Classification
Class 1
The first one is the NS3/4A protease inhibitors. For example, Glecaprevir, Paritaprevir, Voxilaprevir, and Grazoprevir. The action of this group or class is the blocking or preventing of a viral protease enzyme that is used in mutation.
Class 2
The second one is nucleoside with nucleotide, which does not have structural protein 5B (NS5B) polymerase blockers. For example, Sofosbuvir. These inhibitors or blockers have an attachment to viral RNA, not allowing it to replicate.
Class 3
The third group or class is protein without structural 5A (NS5A) blockers. NS5A is called a viral protein by blocking which the virus cannot multiply. In this group, we have Ledipasvir, Daclatasvir, Ombitasvir, Pibrentasvir, and Elbasvir.
Class 4
Non-nucleoside preventers of NS5B polymerase. For example, Dasabuvir includes themselves in the hepatitis C virus foremost to stopping virus imitation (Poordad et al., 2012).
DAAs be supposed to join or with PEG-interferon or RBV to improve the antiviral outcome and SVR rates. DAAs considerably enhanced the cure of the hepatitis C virus fewer times and with minor unwanted effects. Therefore, the WHO preferred the broad utilization of DAAs for facilitating hepatitis C patients in the entire world from getting this treatment and better life. Though, the present limits of DAAs like complicated access to get these therapies led to the appearance of resistance of viral because of increased mutation rate and hazards of developing few deleterious effects, for example, hepatocellular carcinoma, leading to the development of another Hepatitis C therapy, which is called as HTAs.
Host Targeting Antivirals
HTAs were appeared to target the deficiency of DAAs. HTAs are examined to be capable of treatment for HCV illness (Zeisel et al., 2013).
HTAs work by obstructing the enzyme’s host and cellular agents needed for the HCV life cycle (Zeisel et al., 2013). Strong anti-HCV action has been introduced by prohibiting HCV access by anti-CD81, anti-SRBI monoclonal antibodies, EGFR inhibitor (erlotinib), or NPC1L1 inhibitor (ezetimibe) (Meuleman et al., 2008). Cyclophilin A (CypA) blockers (Alisporivir/Debio 025, SCY-635 and NIM811) as well interrupt the multifaceted of CypA-NS5A, prohibiting HCV repetition and increasing the response of immune to virus blockers (Chapel et al.,2006). Alpha-glucosidase inhibitors (for example, MX-3253) obstruct HCV assemblage through the wrong folding of the virus envelope glycoproteins (Chapel et al., 2007). Because of affecting on cellular target, which has related to short transmutation, HTAs have high level inherited barriers for resistance.
HCV Vaccination
Global Health Sector Strategy on hepatitis virus (2016–2021) wished to radically diminish the new HCV diseases by 90% in 2030, which thusly requires moderate admittance to efficient treatment choices everywhere in the world. Regardless of the continuous examination on the treatment of HCV contaminated patients, there is not yet a major demand for a vaccine against this infection to avoid the danger of sickness transmission between people.
As most vaccines focus on the external surface of infections to create antibodies, the HCV vaccine is trying because of the high heterogeneity, hereditary inconstancy, and high transformation rate (Jawaid et al., 2008). This translate or work out that why there are no accessible vaccines of commercial against HCV, which was distinguished since 1989.
Ongoing understanding of HCV structure and development of some preserved natural resistance stimulating parts of the virus (for example, 5and 3UTR) brought about likelihoods of vaccination against HCV. Candidates for reasonable HCV antibodies should be able to activate intense and delayed humoral and immune reactions of cells toward various genotypes of the infection and infection spread between cells (Ippolito et al., 2015). Furthermore, preventive vaccines should have the option to activate the creation of nAbs to resist the infection from arriving at target cells (Burton et al., 2012).
HCV immunization could be drawn nearer using prophylactic or helpful (as an aide to HCV antiviral treatment) antibodies. Old style vaccines, which are set up from the entire infection (inactivated or lessened), are not prescribed with HCV because of biohazard concerns. In any case, the consideration was paid to the utilization of new methodologies of vaccination consisting of recombinant proteins (for example, recombinant Hepatitis C virus E1 and E2 proteins, recombinant HCV centre and NS3-NS4-NS5A-NS5B proteins) (Polakos et al., 2001), manufactured peptides (Klade et al., 2008), dendritic cells, virosome-based antibodies and DNA based vaccines (Puig et al., 2006) to create a protected vaccine. These new vaccine approaches are yet under clinical preliminaries. Besides, the HCV vaccine could be intended to have various epitopes to activate a solid multi-resistant reaction (Chattergoon et al., 1997; Zeng et al., 2009).
Vaccine Updates
A protection vaccine is required to stop the spread of HCV to non-infected people; also, the individuals got relieved through DAA yet stay in danger for re-establishment and diligence of infection. Main barriers to Hepatitis C virus antibody advancement include infection’s variety, infection’s capacity for avoiding resistant reaction in contaminated people having higher paces of transformation (Moradpour et al., 2016).
Despite these difficulties, a few examinations have shown accomplishment in the preclinical creature, which considers indicating enlistment of both humoral and cell insusceptibility against HCV. (Folgori et al., 2006).
Promising primer outcomes have been exhibited in preliminaries led in people situated to some extent on these findings. (Swadling et al., 2014) accordingly, a stage II human clinical preliminary.
Forthcoming Outlooks of Nanomedicines Based HCV Treatments
HCV is a global problem of suffering that has impacts on millions of populations with a bad outcome on health, social, and economic improvement. Because of the finding of the HCV in1989, there is an appearance of an enormous number of the latest therapies capable of providing HCV patients with a recovered life. With the capability to combine and integrate apparatus, nanotechnology offers a potent involvement to the upcoming of HCV avoidance, analysis, and curing by conducting specific characteristics to the medicines. These specific characteristics involve exterior functionality with one or more targeted ligands, conducting high specificity, affinity to liver cells, and as a result, off-target buildup, which leads to very low unwanted effects (Park et al., 2016; Abd Ellah et al., 2019; Craparo et al., 2013). Alternatively, the nano process’s capacity to address over one curative half could be the reason for the polyvalent medication and restricted release actions.
Moreover, HCV gene treatment, utilizing siRNA, would not be effective without a nanocarrier, which can proficiently condensate and convey intact genetic materials to their objectives, influencing the virus life cycle.
Nanomedicine, which can guard and control the destiny of the encapsulated drug, has colossal capacities to draw an away from HCV treatment through conquering a few difficulties. A portion of these difficulties incorporates viral obstruction, patient admittance to viable treatment, shortening the period of treatment, and accessibility of prophylactic vaccines to avoid the additional spread of HCV.
Development of HCV obstruction stays for the second as a significant test to survive. Productive DAAs monotherapy could be impeded because of its low hereditary hindrance to obstruction (McCown et al., 2008), which requires searching for new treatment regimens. Notwithstanding, nanosystems, which can house more than one helpful moiety, could undoubtedly convey diverse HCV combination treatments, diminishing the danger of treatment disappointment (Lee et al., 2018). Then again, considering the instrument of activity, HTAs have a higher hereditary obstruction to the opposition than DAAs. Many of these HTAs are hereditary materials, which need promising nanocarriers to be effectively conveyed to their objectives, defeating DAA deficiencies.
Corresponding to the advancement of effective HCV treatment, worldwide disposal of the infection relies additionally upon decreasing the expense of these treatments and improving the patient's admittance to these medications. The proposed nanosystems are foreseen to lessen the epitomized portion while keeping on adequate medication viability (Ventola, 2017). Diminishing the portion of costly medications will bring about a decrease of the all-out creation cost, and thusly, treatment will be reached out to all HCV patients.
The current 6-week treatment is of a long period, and shortening to about a month or less to improve patient compliance appears to be a challenge (Deterding et al., 2016). Encapsulation of anti - HCV agents inside surface-adjusted and functionalized nanosystems brings about streamlined medication dosing and upgraded delivery to the objective site (Abd Ellah & Abouelhmagd, 2017). Surface-functionalization with a certain focusing on moieties can coordinate the enemy of HCV containing nanosystem toward liver cells, where the virus mostly multiplies. It is accepted that with designed nanosystems bearing moieties to focus on its conveyance, there is a would like to abbreviate treatment term for all HCV populaces.
Numerous HCV patients are ignorant of their disease and are considered as a primary supply for infection, particularly among youthful people who infuse drugs (Ryoo et al., 2012). Utilizing nanotechnology, a prophylactic vaccine, which was not accessible till now and is viewed as a need to forestall additionally spread of the infection all around the world, could be drawn nearer.
Because of these broad examinations and hopeful results, hostile to HCV nanomedicine is considered a promising future treatment for HCV disease.
Worldwide and Hazard Based Hepatitis
The recognizable proof of hazardous factors related to diminishing Hepatitis C disease led to the hazard-based hepatitis C screening suggestions given by the US CDC in 1998 (CfDC, 1998). Though delicate for the people’s identifications with ongoing HCV disease, danger-based screening would not recognize most people with HCV disease due to both barriers of clinician and patients. (Kuncio et al., 2015). Analysis of the 2003-2010 National Health and Nutrition Examination Survey's predominance information illustrated that roughly third-fourth of people with persistent HCV in the US would come under the 1945-1965 birth group (Kabiri et al., 2014). Based on these statistics, CDC and USPSTF suggested all people’s 1-time hepatitis C screening in this birth regiment (1945-1965) paying little heed to risk factors. (Moyer & V. A., 2013; Smith, 2012). The occurrence of HCV expanded from 2010 to2017 (Ghany et al., 2019). The increase in the acute Hepatitis C virus contamination rate has been an increase every year from 2009 to 2017. A greater part of these new Hepatitis C virus infections arisen in people brought into the world after 1965, with those aged 20-39 years representing most of the cases. Numerous modeling examines propose the efficiency of cost of such an approach (Eckman et al., 2019). As a result, the AASLD–IDSA guidance, Hepatitis C virus screening, and subsequent proposals were modernized and incorporate suggested worldwide Hepatitis C virus screening for all grown-ups matured eighteen ages or more surveyed by intermittent testing for people with ongoing hazard practices and introductions.
Conclusion
HCV has globally infected millions of individuals with negative outcomes on individuals’ health, social, and economic life. In the field of diagnosis of HCV, technology is changing at a rapid pace, and one of the major goals is to have a quick HCV diagnosis, easy to use and less expensive. The latest therapies, albeit effective and noted a decrease in rates of mortality and morbidity due to the advancements but still have adverse side effects. The advancements in the medical sciences have made it possible to cure the infection, and most people now can live with a normal life expectancy. The electrochemical immunosensor and Geno sensors have been proved as the most effective approaches in the therapy of HCV. Among them, nontechnology has played a vital role and contributed to biomedicine in the recent era. It is also considered to be a more promising treatment tool in the coming years. In a nutshell, we can say that nanomedicine is a pressing need for HCV treatment. As noted above, there are still adverse side effects of the latest therapies, and it requires a lot of work to be done in the management and way of treatment to this chronic disease. Apart from that, we should not forget the important factor of raising awareness among the masses; as infected syringes and blood, contact is still the highest cause of increased infection rate.?
References
Cite this article
-
APA : Zehussain, S., Ilyas, M., & Ahmad, A. (2017). Advancements in the Diagnostic and Treatment Approaches of Hepatitis C Virus. Global Immunological & Infectious Diseases Review, II(I), 28-40. https://doi.org/10.31703/giidr.2017(II-I).03
-
CHICAGO : Zehussain, Sameena, Muhammad Ilyas, and Ayesha Ahmad. 2017. "Advancements in the Diagnostic and Treatment Approaches of Hepatitis C Virus." Global Immunological & Infectious Diseases Review, II (I): 28-40 doi: 10.31703/giidr.2017(II-I).03
-
HARVARD : ZEHUSSAIN, S., ILYAS, M. & AHMAD, A. 2017. Advancements in the Diagnostic and Treatment Approaches of Hepatitis C Virus. Global Immunological & Infectious Diseases Review, II, 28-40.
-
MHRA : Zehussain, Sameena, Muhammad Ilyas, and Ayesha Ahmad. 2017. "Advancements in the Diagnostic and Treatment Approaches of Hepatitis C Virus." Global Immunological & Infectious Diseases Review, II: 28-40
-
MLA : Zehussain, Sameena, Muhammad Ilyas, and Ayesha Ahmad. "Advancements in the Diagnostic and Treatment Approaches of Hepatitis C Virus." Global Immunological & Infectious Diseases Review, II.I (2017): 28-40 Print.
-
OXFORD : Zehussain, Sameena, Ilyas, Muhammad, and Ahmad, Ayesha (2017), "Advancements in the Diagnostic and Treatment Approaches of Hepatitis C Virus", Global Immunological & Infectious Diseases Review, II (I), 28-40
-
TURABIAN : Zehussain, Sameena, Muhammad Ilyas, and Ayesha Ahmad. "Advancements in the Diagnostic and Treatment Approaches of Hepatitis C Virus." Global Immunological & Infectious Diseases Review II, no. I (2017): 28-40. https://doi.org/10.31703/giidr.2017(II-I).03